Skip to content
Skip to content
Introduction:
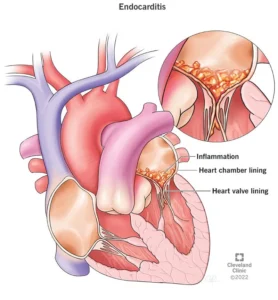
Infective endocarditis (IE) is a serious and potentially life-threatening condition characterized by the infection of the inner lining of the heart chambers and heart valves. This condition can affect both native heart valves, which a person is born with, and prosthetic heart valves, which are artificial replacements for damaged valves. In this article, we will delve into the nuances of infective endocarditis, its causes, risk factors, clinical presentation, diagnosis, and treatment options for both native and prosthetic heart valves.
Infective Endocarditis in Native Heart Valves: Infective endocarditis affecting native heart valves occurs when bacteria or other infectious agents enter the bloodstream and attach to the heart’s natural valves. These microorganisms can damage the heart valve tissue, causing inflammation and potentially leading to valve dysfunction.
Causes and Risk Factors:
- Bacteria are the most common culprits behind infective endocarditis. Streptococci and Staphylococcus aureus are frequently implicated.
- Individuals with pre-existing heart conditions, such as mitral valve prolapse, are at a higher risk.
- Intravenous drug users and those with a history of heart surgeries also face an increased risk.
Clinical Presentation:
- Symptoms may vary but commonly include fever, fatigue, night sweats, and unexplained weight loss.
- Heart murmur, which is an abnormal heart sound, is a frequent finding.
- Complications like septic emboli (small infected masses that travel through the bloodstream) can lead to organ damage.
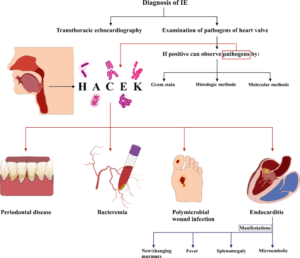
Diagnosis:
- Blood cultures are crucial in identifying the causative microorganisms.
- Echocardiography, both transthoracic and transesophageal, helps visualize the heart valves and detect any abnormalities.
Treatment:
- Intravenous antibiotics are the mainstay of treatment, tailored to the specific bacteria causing the infection.
- Hospitalization might be necessary for severe cases, where close monitoring is essential.
II. Infective Endocarditis in Prosthetic Heart Valves: Prosthetic heart valves, though life-saving, can also be susceptible to infective endocarditis due to their foreign material that can attract bacteria.
Causes and Risk Factors:
- The risk is higher in the early months following valve replacement surgery.
- Dental procedures, surgeries, or infections in other parts of the body can introduce bacteria into the bloodstream.
Clinical Presentation:
- Similar to native valve IE, symptoms can include fever, fatigue, and heart murmur.
- Patients may experience new or worsening heart failure.
Diagnosis:
- Blood cultures remain essential for identifying the causative microorganisms.
- Echocardiography, especially transesophageal, provides detailed images of the prosthetic valve.
Treatment:
- Aggressive antibiotic therapy is the standard approach, often requiring longer courses than in native valve cases.
- In some instances, surgical removal of the infected valve might be necessary.
Prevention:
- Antibiotic prophylaxis before dental and surgical procedures may be recommended for those at high risk.
- Maintaining good oral hygiene and promptly treating infections can help minimize the risk.
Conclusion: Infective endocarditis, whether affecting native or prosthetic heart valves, demands prompt diagnosis and appropriate management to prevent complications. Awareness of risk factors, timely medical attention, and adherence to preventive measures are essential to mitigate the impact of this potentially life-threatening condition. If you suspect any symptoms or risk factors, consult a healthcare professional promptly to ensure early intervention and a positive outcome.
Specific Organisms and Therapeutic Regimens
Organism-specific regimens for infective endocarditis are provided below, including those for Staphylococcus aureus, Streptococcus, Enterococcus, HACEK organisms (Haemophilus parainfluenzae, Haemophilus aphrophilus, Haemophilus paraphrophilus, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella species), Q fever endocarditis, culture-negative endocarditis, and Brucella.
Staphylococcus aureus
Native valve endocarditis (NVE)
Methicillin-susceptible
- Nafcillin 12 g IV q24h in 4-6 divided doses for 6 weeks (optional: gentamicin 3 mg/kg IV or IM q24h in 2-3 divided doses for 3-5 days; however, the benefit of low-dose aminoglycoside is low and nephrotoxicity is a risk; gentamicin is not recommended for treatment of right-sided staphylococcal NVE)
- Cefazolin 6 g IV q24h in 3 divided doses for 6 weeks (optional: gentamicin 3 mg/kg IV or IM q24h in 2-3 divided doses for 3-5 days) for non-anaphylactoid penicillin allergy.
Methicillin-resistant, penicillin-intolerant, or coagulase-negative staphylococci
- Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks (rifampin 300-600 mg q12h may be added; gentamicin should not be added to vancomycin for native valve endocarditis treatment); vancomycin trough between 15 and 20 mcg/mL
- Daptomycin ≥8 mg/kg/dose for 6 weeks for normal renal function may be an alternative to vancomycin to treat left-sided MRSA endocarditis.
Patients with unstable renal function
- Linezolid 600 mg IV q12h; note that linezolid is not yet recommended in guidelines, although there are anecdotal reports of successful treatment with linezolid in gram-positive endocarditis in patients with limited treatment options.
Duration of therapy
- 2 weeks for uncomplicated right-side staphylococcal endocarditis in patients with a history of injection drug use
- 6 weeks for complicated right-side staphylococcal endocarditis.
Prosthetic valve endocarditis (PVE)
Consideration should be given to early surgical intervention.
Methicillin-susceptible
- Nafcillin 12 g IV q24h in 6 divided doses for ≥ 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 2-3 divided doses for 2 weeks plus rifampin 900 mg IV or PO q24h in 3 divided doses for ≥ 6 weeks
- If the organism is gentamicin resistant, then other aminoglycosides may be used depending on susceptibility
- If the organism (especially coagulase-negative Staphylococcus) is resistant to all aminoglycosides, substitute a fluoroquinolone with other 2 drugs for the entire course of therapy
- If the organism is both aminoglycoside and fluoroquinolone resistant, then linezolid, cefatrizine, or trimethoprim-sulfamethoxazole can be used for the first 2 weeks of treatment.
Methicillin-resistant
- Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus rifampin 900 mg IV or PO q24h in 3 divided doses for ≥ 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 2-3 divided doses for 2 weeks
- In patients with fluctuating renal function, consider linezolid 600 mg q12h or ceftaroline 600 mg q12h; for both, clinical experience is very limited
- Patients failing therapy on vancomycin, if fever or symptoms persist, or for breakthrough bacteremia, vancomycin susceptibility testing should be done; vancomycin in such cases should be substituted for daptomycin >8 mg/kg/24 h, which has been approved for the treatment of S aureus BSI and right-sided infective endocarditis; higher doses of daptomycin 12 mg/kg/24 h have also been used ; patients who have received vancomycin have a higher rate of resistance to daptomycin.
- Methicillin-resistant S aureus (MRSA) with vancomycin minimal inhibitory concentration (MIC) >1.0: Telavancin or daptomycin with nafcillin or ceftaroline has been used.
Streptococcus
Native valve endocarditis
Highly penicillin-susceptible viridans group streptococci and Streptococcus gallolyticus (bovis) (MIC ≤ 0.12)
- Aqueous penicillin G 12-18 million U IV q24h continuously or in 4-6 divided doses for 4 weeks or
- Ceftriaxone 2 g IV or IM q24h in 1 dose for 4 weeks if the isolate is ceftriaxone susceptible or
- Aqueous penicillin G 12-18 million U IV q24h continuously or in 4-6 divided doses for 2 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 2 weeks or
- Ceftriaxone 2 g IV/IM q24h in 1 dose for 2 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 2 weeks
- If patient is penicillin or cephalosporin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 4 weeks.
Relatively penicillin-resistant viridans group streptococci or S bovis (MIC > 0.12 and < 0.5)
- Aqueous penicillin G 24 million U IV q24h in 4-6 divided doses for 4 weeks plus gentamicin 3 mg/kg IV q24h in 1 dose for 2 weeks or
- Ceftriaxone 2 g IV/IM q24h in 1 dose for 4 weeks plus gentamicin 3 mg/kg IV q24h in 1 dose for 2 weeks
- If patient is penicillin or cephalosporin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 4 weeks.
Penicillin-resistant viridans group streptococci and S bovis (MIC ≥ 0.5)
- Ampicillin 12 g IV q24h in 6 divided doses for 4-6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 4-6 weeks or
- Aqueous penicillin G 18-30 million U IV q24h in 2 divided doses for 4-6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 4-6 weeks.
- If patient is penicillin or cephalosporin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 6 weeks.
- Streptococcus pneumoniae can cause valve-damaging endocarditis. For penicillin-susceptible strains: Penicillin G 24 million units per day is used. Other penicillin-resistant strains may respond only to vancomycin. Other streptococcal species (e.g., groups A, B, C, and G) may be relatively penicillin-resistant. They are treated by adding gentamicin to a penicillin or cephalosporin for the first 2 weeks of 4- to 6-week therapy.
Prosthetic valve endocarditis
Penicillin-susceptible viridans group streptococci or S bovis (MIC ≤ 0.12)
- Aqueous penicillin G 24 million U IV q24h continuously or in 4-6 divided doses for 6 weeks with or without gentamicin 3 mg/kg IV or IM q24h in 1 dose for 2 weeks or
- Ceftriaxone 2 g IV or IM q24h in 1 dose for 6 weeks with or without gentamicin 3 mg/kg IV or IM q24h in 1 dose for 2 weeks.
- If patient is penicillin or cephalosporin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks.
Penicillin relatively or fully resistant (MIC > 0.12)
- The American Heart Association recommends continuing aminoglycosides for the entire course of treatment (4-6 weeks).
- Aqueous penicillin G 24 million U IV q24h continuously or in 4-6 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 6 weeks or
- Ceftriaxone 2 g IV or IM q24h in 1 dose for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 6 weeks or
- If patient is penicillin or cephalosporin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks.
Enterococcus
Native or prosthetic valve endocarditis
Penicillin, gentamicin, and vancomycin susceptible
- Ampicillin 12 g IV q24h in 6 divided doses for 4-6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 4-6 weeks or
- Aqueous penicillin G 18-30 million U IV q24h continuously or in 6 divided doses for 4-6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 4-6 weeks.
- If patient is penicillin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 6 weeks.
Penicillin, streptomycin, and vancomycin susceptible; gentamicin resistant
- Ampicillin 12 g IV q24h in 6 divided doses for 4-6 weeks plus streptomycin 15 mg/kg IV or IM q24h in 2 divided doses for 4-6 weeks or
- Aqueous penicillin G 18-30 million U IV q24h continuously or in 6 divided doses for 4-6 weeks plus streptomycin 15 mg/kg IV or IM q24h in 2 divided doses for 4-6 weeks.
- If patient is penicillin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus streptomycin 15 mg/kg IV or IM q24h in 2 divided doses for 6 weeks.
Beta-lactamase producing; vancomycin and aminoglycoside susceptible
- Ampicillin-sulbactam 12 g IV q24h in 4 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 3 divided doses for 6 weeks.
- If patient is penicillin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 6 weeks.
Intrinsic penicillin resistance
- Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 1 dose for 6 weeks.
Penicillin, gentamicin, and vancomycin resistant
- Infectious disease consultation recommended. Optimal therapy for VRE PVE has not been clearly defined. Daptomycin and linezolid susceptibility should be obtained.
- VRE: Enterococcus faecium or Enterococcus faecalis: Linezolid 1200 mg IV or PO q24h in 2 divided doses for ≥ 6 weeks or
- Daptomycin 10-12 mg/kg per dose for ≥6 weeks
HACEK organisms
Native or prosthetic valve endocarditis
- Ceftriaxone 2 g IV or IM q24h in 1 dose for 4 weeks for NVE, 6 weeks for PVE or
- Ampicillin-sulbactam 2 g IV q4h for 4 weeks for NVE, 6 weeks for PVE if isolate is susceptible
- If patient is penicillin or cephalosporin intolerant: Ciprofloxacin 1000 mg PO or 800 mg IV q24h in 2 divided doses for 4 weeks for NVE and 6 weeks for PVE.
Corynebacterium (diphtheroid)
Native or prosthetic valve endocarditis
- Penicillin as for streptococci with gentamicin (for MIC < 4 mcg/mL).
- Vancomycin is bactericidal for diphtheroid; for penicillin-allergic or gentamicin-resistant patients, vancomycin can be used.
Gram-negative bacilli
Native or prosthetic valve endocarditis
- Pseudomonas aeruginosa endocarditis, especially if prosthetic valves or left-sided requires consideration for surgical excision.
- P aeruginosa endocarditis can be medically treated, especially native valve, with tobramycin 2.5 mg/kg IV q8h, (peak should be 15-20 mcg/mL and trough concentration should be 2 mcg/mL) plus piperacillin 4 g IV q4h or ceftazidime 2 g IV q8h for 4-6 weeks.
- Alternatively, aztreonam, ciprofloxacin, or imipenem, each with gentamicin, tobramycin, or amikacin depending on susceptibilities.
Fungi
- For Candida endocarditis, amphotericin B lipid formulation 0.8-1 mg/kg/d IV for at least 6 weeks plus flucytosine (5-FC) 25 mg/kg/day divided in 4 doses for normal renal function plus surgery depending on clinical condition and other factors or
- Echinocandins: caspofungin 150 mg/day, micafungin 150 mg/day, or anidulafungin 200 mg/day
Prosthetic valve endocarditis
- Surgical excision of prosthetic valve, in addition to above
- Relapse is high in Candida endocarditis, even with surgical excision, and fluconazole 400-800 mg recommended for prolonged period after surgery or lifelong, if susceptible
Culture-negative endocarditis
Native valve endocarditis
- Ampicillin: 12 g IV q24h in 4 divided doses for 4-6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 3 divided doses for 4-6 weeks
- If patient is penicillin intolerant: Vancomycin 30 mg/kg IV q24h in 2 divided doses for 4-6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 3 divided doses for 4-6 weeks plus ciprofloxacin 1000 mg IV or IM q24h in 2 divided doses for 4-6 weeks
Prosthetic valve endocarditis (≤ 1y after implantation)
- Vancomycin 30 mg/kg IV q24h in 2 divided doses for 6 weeks plus gentamicin 3 mg/kg IV or IM q24h in 3 divided doses for 2 weeks plus cefepime 6 g IV q24h in 3 divided doses for 6 weeks plus rifampin 900 mg PO or IV q24h in 3 divided doses for 6 weeks
Prosthetic valve endocarditis (> 1y after implantation)
- Same regimen as for patients with culture-negative native valve endocarditis, with the addition of rifampin 900 mg PO or IV q24h in 3 divided doses for 6 weeks
Miscellaneous organism-specific treatment
Brucella endocarditis
Brucella infective endocarditis is treated with an aminoglycoside, doxycycline, and rifampin for 6 weeks to 6 months in various regimens, as follows: [16, 17]
- Doxycycline 100 mg IV q12h with
- Streptomycin 1 g IM daily for 14-21 days or gentamicin 5 mg/kg IV daily for 7-10 days or
- Doxycycline with rifampin 600 or 900 mg orally once daily, both for 6 weeks
Q-fever endocarditis due to Coxiella burnetiid
Q fever endocarditis requires at least 18 months of therapy with the following: [18, 19]
- Doxycycline 200 mg daily plus hydroxychloroquine 600 mg daily or
- Doxycycline plus ciprofloxacin (1500 mg/day) or ofloxacin (600 mg/day) or
- Doxycycline (200 mg/day) plus rifampin (900 mg/day)
References
1, The heart .org
2, medscape.com